Zheng-Chun Zhou,
Qiong Zhang,
Zhi-Wei Zhao,
Jian-Jun Ge ![]()
For correspondence:- Jian-Jun Ge Email: anyidage@126.com Tel:+8655162922042
Received: 4 February 2015 Accepted: 11 December 2015 Published: 31 March 2016
Citation: Zhou Z, Zhang Q, Zhao Z, Ge J. Autoimmune response confers decreased cardiac function in patients with rheumatic mitral lesion following valve replacement. Trop J Pharm Res 2016; 15(3):657-662 doi: 10.4314/tjpr.v15i3.31
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To explore the effect of autoimmune response on the decreased cardiac function in patients with rheumatic mitral lesion following valve replacement.
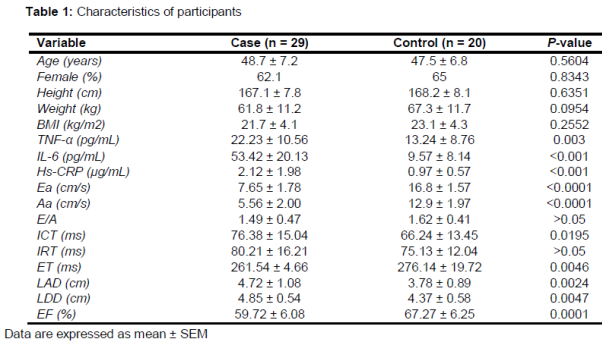
Methods: In this case-controlled study, 29 patients who had undergone valve replacement as a result of mitral lesion were enrolled (mean age = 48.7 years). Twenty healthy volunteers were selected as control (mean age = 47.5 years). Plasma levels of tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), high –sensitivity C-reactive protein (hs-CRP) and echocardiographic indices of heart function in the two groups were investigated, respectively. Body mass index (BMI) was also calculated.
Results: TNF-α, IL-6 and hs-CRP levels in plasma were significantly higher than those in controls (p < 0.05; 22.23 pg/mL vs. 13.24 pg/mL, 53.42 pg/mL vs. 9.57 pg/mL, and 2.12 μg/mL vs. 0.97 μg/mL, respectively). The indices of left atrial diameter (LAD), left ventricular end-diastolic diameter (LDD) and isovolumetric contraction time (ICT) were significantly higher (p < 0.05; 4.72 cm vs. 3.78 cm, 4.85 cm vs. 4.37 cm, and 76.38 ms vs. 66.24 ms, respectively), but those of early diastolic velocity (Ea), late diastolic velocities (Aa) and ejection time (ET) were significantly lower (p < 0.05; 7.65 cm/s vs. 16.8 cm/s, 5.56 cm/s vs. 12.9 cm/s, and 261.54 ms vs. 276.14 ms, respectively). Two-dimensional echocardiography obtained the same results.
Conclusion: Valve replacement in patients with rheumatic heart disease (RHD) does not attenuate inflammatory response; rather, autoimmune response would keep affecting decreased heart function in RHD patients who have received mitral valve replacement.
Introduction
Rheumatic fever (RF) is a delayed consequence of throat infection by Streptococcus pyogenes, and often affects susceptible untreated children. Nearly 30 - 45 % of the affected children could develop progressive and permanent valvular lesions, and leading to rheumatic heart disease (RHD). There are 15.6 million new cases of RHD per year worldwide, resulting in 233,000 deaths per year in developing countries [1]. The epidemiological data demonstrated that RHD is a crucial health problem.
Currently, the mechanism of RHD is still far from being understood. The pathogenesis of RHD is complex, and potential reasons include cellular responses of Streptococcus pyogenes and autoimmune humoral responses toward human tissues [2]. The mechanism of molecular mimicry is the process whereby T cells recognize self-antigens, mainly the M protein of heart tissue, which shares homology with streptococcal antigens. Once activated, the T cells from RHD patients were able to recognize streptococcal M protein peptides as well as myocardium and valvular proteins, resulting in valvular lesions [3]. According to this pre-supposition, the process of autoimmune response should be eradicated after valve replacement by removing the valvular proteins and the heart function of RHD patients should be recovered. However, increasing clinical evidences indicated that the painful symptom still existed in most RHD patients after valve replacement. Therefore, mechanism of this phenomenon still remains uncertain.
It has been noted that the autoimmune response status can be reflected by evaluating the cytokines’ levels [4]. A large number of studies have demonstrated that the production of inflammatory cytokines, including tumor necrosis factor (TNF)-α, interleukin (IL)-6 and high-sensitivity C-reactive protein (hs-CRP), were increased after streptococcal antigen and pokeweed mitogen stimulation [5]. Therefore, the elevated levels of TNF-α, IL-6 and hs-CRP appear to play critical roles in triggering immunological and inflammatory reactions of RHD patients. In this study, it was hypothesized that the autoimmune response would persistently exist in RHD patients who have received heart valve replacement.
Clinically, two-dimensional echocardiography is widely used as an effective approach to evaluate cardiac function heart function of patients with RHD [6], thus the echocardiographic indices were measured to evaluate the heart function, and the plasma levels of TNF-α, IL-6 and hs-CRP were detected to investigate whether the autoimmune response affect the RHD patients receiving valve replacement or not. Also, the relationship between the plasma levels of TNF-α, IL-6, CRP and echocardiographic indices were analyzed to further explore the pathogenesis mechanism of the RHD patients who have received heart valve replacement.
Methods
Subjects and study protocol
One thousand and five patients had undergone mitral valve replacement during January 2008 to May 2010 at the First Affiliated Hospital of Anhui Medical University. Of which, twenty-nine patients (mean age = 48.7 ± 7.2 years) were selected in this study. Rheumatic mitral lesions in the patients prior to operation were evaluated based on the clinical classification of New York Heart Association (NYHA). Six of the 29 selected patients were classified as NYHA class II, fifteen as class III, and eight as class IV. The operations were performed by the identical surgeons in the hospital.
The instrumental prosthetic valves implanted were provided by Sorin Group (Italian). Heart function of the patients was recovered to NYHA class I after valve replacement. Additional 20 healthy volunteers were recruited as the controls and were matched by age and gender (mean age = 47.5 ± 6.8 years). Subjects from either group were excluded if they had a history of cerebrovascular events, hyperlipidemia, venous thrombosis, diabetes, pulmonary diseases, disease of immune system, degenerative neurologic disorders, renal or liver disease, acute rheumatic fever, acute infection, inflammatory disease, malignancy, acute myocardial infarction, recent major surgery, trauma, and other chronic cardiovascular diseases such as hypertension and coronary heart disease.
Informed consents were obtained from all study patients. Weight was measured to the nearest 0.1 kg and calibrated with known weights and height was measured to the nearest 0.1 cm by using a stadiometer at the enrollment into the department of Cardiovascular Surgery in the First Affiliated Hospital of Anhui Medical University. Body mass index (BMI; kg/m2) was calculated.
The patients continued treatment with digoxigenin, anticoagulant and diuretic for three months after the operation. The time course from the valve replacement surgery to the enrolment in this study was 3-29 months, and the average time was 15.3 months. The study protocol was approved by the Institutional Ethic Committee, Anhui Medical University (no. AHM-2007105#).
Measurement of TNF-α and IL-6
Blood samples of the patients were collected into an evacuated tube containing 3.8 % buffered sodium citrate. Plasma fractions were obtained by centrifugation for 10 min at 2000 rpm at room temperature, and aliquots were prepared and stored at −80 °C until the assay. Plasma levels of TNF-α and IL-6 were measured according to the manufacturer protocols of ABC-ELISA (R&D).
Measurement of hs-CRP
Hs-CRP was measured by latex-enhanced immunoturbidimetric assay with automatic biochemistry analyzer (ADVIA Chemistry System, Bayer HealthCare AG, Leverkusen, Modular-P Switzerland). Both antiserum and standard substance were supplied by the DiaSys Diagnostic Systems Co., Ltd (Shanghai).
Echocardiographic examination
Both the patients and healthy volunteers underwent transthoracic two-dimensional and Tissue Doppler Echocardiographic examination by means of the Philips iE33 system with a 5.0 MHz transducer. All echocardiographic examinations were assessed by an identical skilled cardiologist. Transthoracic echocardiographic measurements were obtained from the parasternal long-axis view by two-dimensional targeted M-mode tracing.
Left ventricular end-diastolic diameter (LDD) and left ventricular ejection fraction (LVEF) were measured to assess the left ventricles function, and left atrial diameter (LAD) was measured to reflect the function of the left atrium. LVEF and LDD were used as the most convenient and sensitive indices to estimate the left ventricular function [7]. Besides, LAD was used to assess the left atrium function [8].
Using the 4-chamber view, a 2-mm sample volume was placed at the lateral corner of the tricuspid valve annulus and early diastolic (Ea) and late diastolic (Aa) myocardial velocities were obtained to evaluate the right heart function. Meanwhile, the indices of E/A, isovolumetric contraction time (ICT), isovolumetric relaxation time (IRT) and Tei index were measured to assess the right heart function. In addition, ECG tracings were performed.
The indices of Ea, Aa, E/A, ET, ICT and IRT were demonstrated to be effective to assess the function of right heart [9, 10]. The Tei index was defined based on the formula: Tei = (ICT + IRT)/ET, to appraise a combined systolic and diastolic right cardiac function [11].
Statistical analysis
The results were expressed as mean ± standard error of the mean (SEM). Analysis of the plasma levels of TNF-α, IL-6 and hs-CRP and the indices of heart function between the cases and the controls were performed using Independent-samples T test. P < 0.05 was considered statistically significant. All analyses were conducted by using statistical software SPSS 13.0.
Results
Plasma levels of TNF-α, IL-6 and hs –CRP in the groups
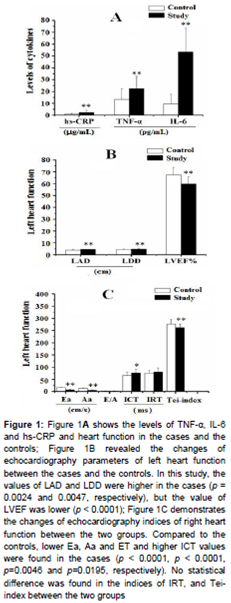
The plasma concentrations of TNF-α, IL-6 and hs-CRP in each group were summarized in . The levels of TNF-α, IL-6 and hs -CRP levels were found to be significantly higher in the cases than in the controls (p < 0.01; 22.23pg/L vs. 13.24 pg/L, 53.42 pg/L vs. 9.57 pg/L, and 2.12 μg/mL vs. 0.97 μg/mL, respectively).
Comparison of two-dimensional echocardio-graphy indices between the cases and control
The echocardiography parameters of the left and right heart function in the two groups were shown in A. Compared with the control group, the indices of LAD and LDD were higher in the cases (p < 0.01, 4.72 cm vs. 3.78 cm and 4.85 cm vs. 4.37 cm respectively), but the value of LVEF (%) was lower (p < 0.0001, B). The indices of Ea, Aa and ET in the cases were significantly lower than those in the controls (p < 0.05; 7.65 cm/s vs. 16.8 cm/s, 5.56 cm/s vs. 12.9 cm/s, and 261.54 ms vs. 276.14 ms, respectively; p < 0.001, p < 0.001 and p < 0.01, respectively), but the index of ICT was higher (p = 0.0195, C). The values for IRT and Tei index in the cases and the controls were similar to each other.
Discussion
In this study, it was found that the levels of TNF-α, IL-6 and hs-CRP in plasma of the cases that received valve replacement were significantly higher than those in the controls. LAD and LDD represented the function of the left atrium, and LVEF indicated the function of the left ventricle. Echocardiography examination results indicated that the heart function was obviously poorer in the cases compared with the controls. The results also indicated that inflammatory process kept affecting the patients received valve replacement. Damaged valves would not be the exclusive source that induced immune reaction in the RHD patients.
Rheumatic fever is autoimmune in nature and results from the production of auto-reactive antibodies and T-cells cross-reactive to the components of group A streptococcus and host tissues. It is evident that T lymphocytes are involved in the pathogenesis of rheumatic carditis, and the previous data supported the hypothesis that antibodies play important roles in the initiation of the disease at the valve endothelium [12]. The elevated levels of pro-inflammatory cytokine are the direct evidences of the presence of the autoimmune reaction. Previous investigations demonstrated that overproduction of TNF-α promoted the induction of post-infection autoimmune response in RHD [13]. The previous data discovered that both the production in the plasma and the expression of TNF-α in the myocardium were significantly higher in patients with rheumatic mitral lesion [14]. Increased serum level of IL-6 occurred in the patients with congestive heart failure [15] and in the patients with RHD [16]. Additional IL-6 might be secreted by the intralesional mononuclear cells from heart lesions predominantly in chronic RHD patients [17]. Moreover, increasing evidences showed CRP was a critical marker in assessing inflammation and tissue injury [18,19]. The plasma concentration of hs-CRP was significantly higher in RHD [20,21] and could reflect progression and outcome of the rheumatic mitral lesion [22]. In this study, it was found that concentrations of TNF-α, IL-6 and hs-CRP in plasma were obviously higher in cases group than those in controls, suggesting excising primary mitral lesions did not obviously enable attenuate the autoimmune response triggered by Streptococcus pyogenes in the cases group.
In previous investigations, there were few studies regarding immune reactions in postoperative patients. In this present study, we focused on whether immune reaction affects the outcome of valve replacement and improvement of cardiac function or not. We found that levels of TNF-a, IL-6 and hs-CRP in plasma were significantly higher in the case groups than those in healthy control groups. The over-production of cytokines could be secreted by T cells in response to autoimmune reaction which caused by the infection of β-hemolytic group A streptococci. Thus, it is advisable to conversely deduce that high levels of the TNF-a, IL-6 and hs-CRP could attribute to the active process of the autoimmune response in patients who undergone valve replacement. In the present research, it was demonstrated that immune reaction in RHD patients would occur even after valve replacement; another potential antigen that induced immune reaction in patients would be prosthetic valve. The mechanical prosthetic valve would act as an allotransplant to elicit the immune reaction [23]. Therefore, it was suggested that the valve replacement could not completely improve the cardiac function of RHD patients. Implementing anti-cytokines (such as anti-IL-6, anti-TNF-α and anti-hs-CRP) and administration of the inhibitor of p38MAPK could be the effective alternative modalities to prevent valve damage in RHD patients and to suppress the immune reaction in the patients received valve replacement.
Conclusion
The cardiac function of RHD patients did not fully recover after valve replacement due to synchronous influence of the autoimmune reaction. The elevated levels of plasma TNF-α, IL-6 and hs-CRP appear to be indices of autoimmune activities. And it seems that the anti-autoimmune therapy administered to group-A streptococcus is an option for RHD patients after valve replacement.
Declarations
Acknowledgement
References
Archives


News Updates